REGULATORY UPDATES
PBM Reform and What It Means for Independent Pharmacy Purchasing in 2026
PBM Reform and What It Means for Independent Pharmacy Purchasing in 2026
PBM Reform and What It Means for Independent Pharmacy Purchasing in 2026
PBM Reform and What It Means for Independent Pharmacy Purchasing in 2026


I remember standing at the counter on a Tuesday afternoon when the month's financial statement came through. I opened the attachment and felt my stomach drop. There it was again: a line item labeled "DIR Fee Clawback." The number was printed right in the middle of the screen, bold and unforgiving. $8,437.
That's the amount the pharmacy benefit manager (PBM) took back from last month's reimbursement because the pharmacy didn't hit some performance metric we didn't even know we was being measured on. It's not a billing error. It's not a mistake. It's how the system works. The PBM sets the rules, moves the goalposts, and then charges me for missing them.
Years behind the counter, I did the mental math that way I did every month: that's part of a technician's salary. That's the MTM initiative we wanted to launch. That's hiring a clinical specialist to deepen patient relationships. It's gone, sent upstream to a PBM that controls which patients we can see, what we can charge, and how much of what we earn, they keep.
If you're reading this, you've probably done that same calculation. You know that feeling. And you might think, "This is just how pharmacy works now." Here's what I want to tell you: It doesn't have to be. And 2026 is actually the year where we're positioned to make real change.
The landscape shifted in 2024 and 2025. Federal regulators woke up. State legislatures started passing real reform bills. And independent pharmacies that are paying attention are already diversifying their purchasing strategies to reduce their dependence on PBM pricing pressure.
Let me show you what's happening, what it means for your pharmacy, and the concrete purchasing strategies that are working right now.
The PBM Problem We All Know But Don't Say Out Loud
Let's start with the structure that created this monster, because you can't fix what you don't understand.
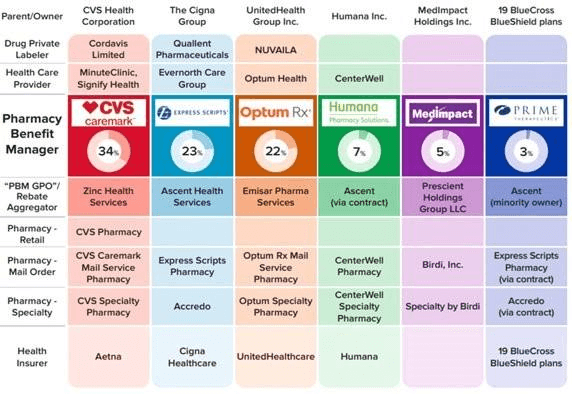
Source: FTC Releases Interim Staff Report on Prescription Drug Middlemen
Three pharmacy benefit managers control about 80% of all prescriptions in America. Let me name them: CVS Caremark, Express Scripts (owned by Cigna), and OptumRx (owned by UnitedHealth). These three companies aren't just middlemen anymore. They're vertically integrated healthcare empires.
CVS Caremark owns CVS Health, CVS pharmacies, and Aetna insurance. Express Scripts is part of Cigna, one of the largest insurers in the country. OptumRx is owned by UnitedHealth, which owns hospitals, clinics, doctors, insurance plans, and data. They're not operating in an industry anymore. They are the industry.
And when a single company owns both the insurance plan and the pharmacy benefit manager and the pharmacy itself, the incentives get twisted in ways that hurt independent pharmacies specifically.
Here's how it actually works, in plain language:
Spread pricing. The PBM tells you they'll reimburse you $50 for a medication. They tell the insurance company it costs $65. They keep the $15 spread. Sometimes the spread is real, based on service costs. Often it's just profit extraction.
DIR fees (Direct and Indirect Remuneration fees). PBMs charge pharmacies for things like "performance metrics," "administrative costs," "patient education resources," "generic incentive programs." These fees often exceed your actual profit margin on those prescriptions. You fill the script at a loss. Then you get charged a fee for the privilege of losing money.
Patient steering. The PBM's formulary directs patients to their own pharmacies or "preferred" network pharmacies. Independent pharmacies get excluded or delisted without warning. Your market shrinks overnight.
Below-cost reimbursement. Some medications are reimbursed below your actual acquisition cost. You lose money on every fill.
Data leverage. The PBM owns the data on what medications work, what patients need, what the market is demanding. They use that data to negotiate with manufacturers and wholesalers in ways that smaller pharmacies can't access.
This structure has been building for 20 years, and it's crushing independent pharmacies at a scale most people don't fully grasp. But something shifted in 2024. Federal regulators started looking at this. And we're now in a moment where reform is actually possible.
Federal Reform Landscape: What Passed, What's Stalled, What's Coming
Let me be honest about what we achieved and what we still need to fight for.
The FTC Interim Report (July 2024). The Federal Trade Commission (FTC) released a comprehensive investigation into the PBM industry. The report found exactly what we've been saying: PBMs are abusing their market power, blocking competition, and harming patients and pharmacies. The FTC called for Congress to act. This wasn't speculation. This was federal investigators confirming what every independent pharmacy owner already knows.
CMS DIR Fee Point-of-Sale Reporting (January 2024). The Centers for Medicare and Medicaid Services (CMS) required PBMs to disclose DIR fees at the point of sale, instead of burying them in monthly statements. This is a small win but a real one. When pharmacists see the actual fee being charged on the screen in real time, they understand the math more clearly.
The PBM Reform Act and the Lower Costs, More Transparency Act. These bills had momentum in Congress. They would have capped DIR fees, banned spread pricing, and required transparent reimbursement. They had bipartisan support. But they stalled. A bill that was expected to pass in December 2024 didn't make it across the finish line. The PBM lobbying effort was significant.
Here's the truth I want us to say out loud together: Federal reform is still coming, but it's not here yet. We can't sit around waiting. We need to act locally and change our purchasing strategy now.
State-Level Victories That Show What's Possible
But here's where it gets interesting, because states are moving faster than Congress.
In 2024, 24 states passed 33 pharmacy benefit manager reform bills. Let me highlight the ones that matter most:
Idaho and Vermont banned spread pricing. Full stop. If you're a PBM in those states, you can't keep the difference between what you charge the patient and what you reimburse the pharmacy. The margin has to be transparent and defensible. This one move cuts off a major revenue stream for PBMs.
Massachusetts. Starting January 2026, pharmacy benefit managers have to get state licensing. They have to meet standards. It's not a ban, but it's oversight. It makes it harder to operate in the shadows.
Alabama's Community Pharmacy Relief Act protects independent pharmacies from sudden delisting and requires PBMs to disclose pricing contracts.
New York passed transparency requirements that are helping independents understand their actual reimbursement.
These state victories matter because they show the model works. When we pressure our state legislators, we get results. When we build campaigns with other pharmacies, we move the needle.
The states winning now are the ones where pharmacy associations got organized. The National Community Pharmacists Association (NCPA) played a major role. Local pharmacy owners showed up at legislative hearings. Patient stories got shared with decision-makers. This wasn't top-down. It was local action creating change.
What This Means for Your Pharmacy's Purchasing Strategy
Okay, so federal reform is in motion. Some states are winning. What do you do Monday morning at your pharmacy?
You diversify. You stop being dependent on one PBM's pricing power. You build redundancy into your sourcing. Here's the framework that's working for independent pharmacies in 2026:
First, data-driven selection of insurance plans.
Not all plans are created equal. Some PBMs are more reasonable on reimbursement. Some have better contracts with your wholesalers. Some have lower DIR fees. You need to know which plans your patients are on and which ones are costing you money.
Pull your claims data from the last 90 days. Segment by PBM. Calculate your average margin per prescription, including DIR fees. You might find that Humana plans reimburse at 3% margin while a Cigna Express Scripts plan reimburses at negative 2%. That's a $5 difference per 100 scripts.
This doesn't mean dropping plans, but it means being strategic about where you focus patient outreach and where you negotiate harder.
Second, aggressive generic cost optimization.
Generics are where most of your volume is, and they're where PBMs apply maximum pricing pressure. But generics also have the most flexibility because there are multiple suppliers and multiple routes to the same medication.
Use multiple wholesalers. National Average Drug Acquisition Cost (NADAC) pricing is published by CMS. You can access it for free. Compare your wholesaler's prices against NADAC. If you're paying 30% above NADAC on a generic, that's a negotiation opportunity.
Work with a pharmacy group or buying group that negotiates national contracts. Group Purchasing Organization (GPO) members get better rates because they have collective buying power.
And this is crucial: leverage pharmacy-to-pharmacy networks like RxPost for those medications where your wholesaler is out of stock or overpriced. RxPost customers get an average 21.8 % discount versus WAC on sourced medications. That's not $1 per script. That's meaningful margin recovery.
Third, build cash reserves specifically for DIR clawback hangover.
This sounds bleak, but it's realistic. Many PBMs aren't changing their fee structures fast enough. You might be dealing with DIR fees for years. Plan for it.
If you're running an average $8,000 to $15,000 monthly DIR costs (which is common for a mid-sized independent), budget for it. Put aside $1,500 to $2,000 per month as cash reserve. It's not pleasant, but it's honest accounting. When reform finally hits and DIR fees drop, that money becomes working capital you can redeploy.
Fourth, data-driven DIR appeals.
PBMs are legally required to provide you with the data behind their DIR fees. If a performance metric doesn't make sense or if the fee seems disproportionate, appeal it. You need documentation: "Our patient fill rate for generic ACE inhibitors was 87%, you're claiming it should be 92%. Show me the data that backs that."
Many PBMs will refund fees if you challenge them with actual documentation. It's not glamorous, but every $1,000 appeal refunded is $1,000 that stays in your business.
Fifth, network with other independent pharmacies on purchasing.
The vertical integration that's crushing us individually is a weakness when we're together. If five independent pharmacies in a region combined their purchasing power, they'd have real leverage with wholesalers and generic manufacturers. Member driven pharmacy associations facilitate this. So do informal pharmacy networks.
Get to know the three or four independent pharmacies closest to you. Share pricing information. Negotiate collective contracts. Buy generic inventory together to hit volume minimums that get you better rates. This is not collusion (that would be illegal). This is collective action for better purchasing terms.
Revenue Diversification: The Real Defense
Here's the hardest truth about PBM pressure: The solution isn't just fighting the PBM in court or lobbying Congress (though we need that too). The solution is making sure script volume and PBM reimbursement aren't 80% of your revenue.
Independent pharmacies winning in 2026 are building a diversified revenue model:
Medication Therapy Management (MTM). The American Pharmacists Association (APhA) and NCPA have resources to get certified. Medicare is expanding MTM payment. You can charge $150 to $300 per patient per year for medication reviews, adherence counseling, safety assessments. A pharmacy with 50 MTM patients generates $7,500 to $15,000 in MTM revenue that's not dependent on PBM reimbursement.
Immunizations. Every independent pharmacy should be offering flu, pneumonia, RSV, and shingles vaccines. Reimbursement is better. Patients appreciate it. It's $25 to $50 per patient per shot. A pharmacy giving 1,000 vaccines a year is generating $25,000 to $50,000 in revenue outside the PBM system.
Diabetes Self-Management Education (DSME). Similar model. Medicare and many commercial plans reimburse. You need certification, but it's achievable. One DSME patient generates $200 to $400 in revenue.
GLP-1 Counseling Services. This is emerging as a huge opportunity. Patients on semaglutide (Wegovy, Ozempic) need counseling on side effects, nutrition, medication interactions. Independent pharmacies that position themselves as GLP-1 counseling centers can charge cash for consultation ($50 to $100) or negotiate reimbursement.
Front-end optimization. This is the non-pharmacy revenue: greeting cards, supplements, OTC pain relievers, vitamins, blood pressure monitors, glucose monitors. Independents can source these more flexibly than chains. Margins are better. And they're not subject to PBM payment.
When 50% of your revenue comes from services and products outside the PBM system, a 10% reimbursement decrease hits differently. You've built redundancy.
Advocacy: Making Your Voice Heard Where It Matters
I could end this article with a framework and tactics. But the most important thing independent pharmacies can do right now is advocacy.
Real reform in states like Alabama, Idaho, and Massachusetts happened because pharmacies showed up and testified. Because patients shared stories about medication access. Because we made the problem visible to elected officials.
Here's what to do this quarter:
Join or increase your NCPA involvement. The NCPA is the national organization actually moving PBM reform legislation. They have regional chapters. Get involved in your chapter. Attend meetings. Participate in letter-writing campaigns.
Contact your state legislators directly. You don't need to be a lobbyist. You're a business owner in their district. Your letter matters. Focus on specific issues: "DIR fees cost our pharmacy $100,000 a year and force us to cut pharmacy tech hours. Is there legislation we can support?" Legislators listen to small business owners.
Share patient stories. When a patient can't get their medication because a PBM delisted your pharmacy, that's a story. When you have to counsel a patient on a less effective medication because their PBM prefers a competitor's drug, that's a story. These stories are more powerful than industry data in legislative meetings.
Join coalitions. In many states, independent pharmacies are joining coalitions with patient advocacy groups, hospitals, and consumer advocates to push for PBM reform. Look up what's happening in your state. Join.
The Oklahoma Pharmacists Association and Arkansas pharmacists have been instrumental in state-level reforms. It's not easy. But it's working.
RxPost: Reducing PBM Dependence Through Diversified Sourcing
Here's the leverage point I keep coming back to because I believe in it: Diversified sourcing reduces PBM power.
When your wholesaler is your only source, and the PBM controls what you can fill, the PBM owns you. When you have multiple sourcing channels, you have options.
RxPost is built on this principle. You connect with 600+ independent pharmacies. When you need medication that your wholesaler is out of stock on or overpricing, you source from peers. You're no longer entirely dependent on one wholesaler's inventory or pricing.
DSCSA compliance is built into the platform. The chain of custody is clean and documented. You're not taking shortcuts.
The economic impact: RxPost customers get an average 21.8% discount versus WAC. That means on a medication your wholesaler is charging $1000 for, you might source it through RxPost at $800. That's margin recovery. That's cash staying in your business instead of going to a wholesaler or PBM.

Average RxPost customers save $12,294 in the first 30 days. They recover $80.8K in surplus inventory value in 60 days. This isn't theoretical. This is happening with independent pharmacies right now.
The philosophical point matters too: When you buy from other independents, you're investing in the network that's actually competing with the chains and the PBMs. You're not strengthening a pharmaceutical distributor or a PBM. You're strengthening your peers.
Make This Actionable
Reform is happening at the federal level, but slower than we need. Reform is winning at the state level, but only in states where pharmacies organized. And you can win at your pharmacy level right now by diversifying your purchasing.
This quarter, take one step: Pull your claims data. Segment by PBM. Find the one that's costing you the most money relative to volume. Make a list of the specific DIR fees or reimbursement issues. Then schedule a meeting with your PBM account manager. Come with data. Ask specific questions. You might be surprised how much room for negotiation exists.
And set up a RxPost account. See what your surplus inventory is worth. See how many prescriptions you could fill from the pharmacy network instead of your wholesaler. This isn't replacing your wholesaler. It's building a second channel.
Take Action This Week
Contact NCPA. Visit ncpa.org. Find your state chapter. Attend a meeting. You're not committing to anything, just getting informed and getting connected.
Pull your claims data. Export your last 90 days of claims by PBM. Calculate your average margin. See where the pressure is coming from.
Create a RxPost account. It's free. List any surplus inventory. See what matches you get in the next 24 hours.
Schedule a PBM conversation. Call your account manager. Don't complain. Come with data. Ask: "Our DIR fees are $X. Can we discuss how those are calculated?"
Next Steps and Resources
The entrepreneurial pharm tech mindset doesn't accept the status quo as inevitable. It asks, "What can I change? What can I control? What leverage do I have?"
PBM reform is one of those moments where the industry is actually shifting. Take advantage of it.
Subscribe to The Entrepreneurial Pharm Tech newsletter for monthly updates on PBM reform, state legislative victories, and purchasing strategies that work. We share what's actually changing and how to position your pharmacy to benefit from it.
Follow RxPost on social (Facebook, Instagram, LinkedIn) for wins from independent pharmacies fighting back against supply chain pressure.
Join your state pharmacy association and NCPA. This is where reform happens.
Connect with us on WhatsApp for questions about purchasing strategy or surplus inventory. We're here to help.
The chains and PBMs want us to believe that this is just how it works. Here's the truth we need to say out loud together: It's not. It's changing. And you have more power than you think.
I remember standing at the counter on a Tuesday afternoon when the month's financial statement came through. I opened the attachment and felt my stomach drop. There it was again: a line item labeled "DIR Fee Clawback." The number was printed right in the middle of the screen, bold and unforgiving. $8,437.
That's the amount the pharmacy benefit manager (PBM) took back from last month's reimbursement because the pharmacy didn't hit some performance metric we didn't even know we was being measured on. It's not a billing error. It's not a mistake. It's how the system works. The PBM sets the rules, moves the goalposts, and then charges me for missing them.
Years behind the counter, I did the mental math that way I did every month: that's part of a technician's salary. That's the MTM initiative we wanted to launch. That's hiring a clinical specialist to deepen patient relationships. It's gone, sent upstream to a PBM that controls which patients we can see, what we can charge, and how much of what we earn, they keep.
If you're reading this, you've probably done that same calculation. You know that feeling. And you might think, "This is just how pharmacy works now." Here's what I want to tell you: It doesn't have to be. And 2026 is actually the year where we're positioned to make real change.
The landscape shifted in 2024 and 2025. Federal regulators woke up. State legislatures started passing real reform bills. And independent pharmacies that are paying attention are already diversifying their purchasing strategies to reduce their dependence on PBM pricing pressure.
Let me show you what's happening, what it means for your pharmacy, and the concrete purchasing strategies that are working right now.
The PBM Problem We All Know But Don't Say Out Loud
Let's start with the structure that created this monster, because you can't fix what you don't understand.
Source: FTC Releases Interim Staff Report on Prescription Drug Middlemen
Three pharmacy benefit managers control about 80% of all prescriptions in America. Let me name them: CVS Caremark, Express Scripts (owned by Cigna), and OptumRx (owned by UnitedHealth). These three companies aren't just middlemen anymore. They're vertically integrated healthcare empires.
CVS Caremark owns CVS Health, CVS pharmacies, and Aetna insurance. Express Scripts is part of Cigna, one of the largest insurers in the country. OptumRx is owned by UnitedHealth, which owns hospitals, clinics, doctors, insurance plans, and data. They're not operating in an industry anymore. They are the industry.
And when a single company owns both the insurance plan and the pharmacy benefit manager and the pharmacy itself, the incentives get twisted in ways that hurt independent pharmacies specifically.
Here's how it actually works, in plain language:
Spread pricing. The PBM tells you they'll reimburse you $50 for a medication. They tell the insurance company it costs $65. They keep the $15 spread. Sometimes the spread is real, based on service costs. Often it's just profit extraction.
DIR fees (Direct and Indirect Remuneration fees). PBMs charge pharmacies for things like "performance metrics," "administrative costs," "patient education resources," "generic incentive programs." These fees often exceed your actual profit margin on those prescriptions. You fill the script at a loss. Then you get charged a fee for the privilege of losing money.
Patient steering. The PBM's formulary directs patients to their own pharmacies or "preferred" network pharmacies. Independent pharmacies get excluded or delisted without warning. Your market shrinks overnight.
Below-cost reimbursement. Some medications are reimbursed below your actual acquisition cost. You lose money on every fill.
Data leverage. The PBM owns the data on what medications work, what patients need, what the market is demanding. They use that data to negotiate with manufacturers and wholesalers in ways that smaller pharmacies can't access.
This structure has been building for 20 years, and it's crushing independent pharmacies at a scale most people don't fully grasp. But something shifted in 2024. Federal regulators started looking at this. And we're now in a moment where reform is actually possible.
Federal Reform Landscape: What Passed, What's Stalled, What's Coming
Let me be honest about what we achieved and what we still need to fight for.
The FTC Interim Report (July 2024). The Federal Trade Commission (FTC) released a comprehensive investigation into the PBM industry. The report found exactly what we've been saying: PBMs are abusing their market power, blocking competition, and harming patients and pharmacies. The FTC called for Congress to act. This wasn't speculation. This was federal investigators confirming what every independent pharmacy owner already knows.
CMS DIR Fee Point-of-Sale Reporting (January 2024). The Centers for Medicare and Medicaid Services (CMS) required PBMs to disclose DIR fees at the point of sale, instead of burying them in monthly statements. This is a small win but a real one. When pharmacists see the actual fee being charged on the screen in real time, they understand the math more clearly.
The PBM Reform Act and the Lower Costs, More Transparency Act. These bills had momentum in Congress. They would have capped DIR fees, banned spread pricing, and required transparent reimbursement. They had bipartisan support. But they stalled. A bill that was expected to pass in December 2024 didn't make it across the finish line. The PBM lobbying effort was significant.
Here's the truth I want us to say out loud together: Federal reform is still coming, but it's not here yet. We can't sit around waiting. We need to act locally and change our purchasing strategy now.
State-Level Victories That Show What's Possible
But here's where it gets interesting, because states are moving faster than Congress.
In 2024, 24 states passed 33 pharmacy benefit manager reform bills. Let me highlight the ones that matter most:
Idaho and Vermont banned spread pricing. Full stop. If you're a PBM in those states, you can't keep the difference between what you charge the patient and what you reimburse the pharmacy. The margin has to be transparent and defensible. This one move cuts off a major revenue stream for PBMs.
Massachusetts. Starting January 2026, pharmacy benefit managers have to get state licensing. They have to meet standards. It's not a ban, but it's oversight. It makes it harder to operate in the shadows.
Alabama's Community Pharmacy Relief Act protects independent pharmacies from sudden delisting and requires PBMs to disclose pricing contracts.
New York passed transparency requirements that are helping independents understand their actual reimbursement.
These state victories matter because they show the model works. When we pressure our state legislators, we get results. When we build campaigns with other pharmacies, we move the needle.
The states winning now are the ones where pharmacy associations got organized. The National Community Pharmacists Association (NCPA) played a major role. Local pharmacy owners showed up at legislative hearings. Patient stories got shared with decision-makers. This wasn't top-down. It was local action creating change.
What This Means for Your Pharmacy's Purchasing Strategy
Okay, so federal reform is in motion. Some states are winning. What do you do Monday morning at your pharmacy?
You diversify. You stop being dependent on one PBM's pricing power. You build redundancy into your sourcing. Here's the framework that's working for independent pharmacies in 2026:
First, data-driven selection of insurance plans.
Not all plans are created equal. Some PBMs are more reasonable on reimbursement. Some have better contracts with your wholesalers. Some have lower DIR fees. You need to know which plans your patients are on and which ones are costing you money.
Pull your claims data from the last 90 days. Segment by PBM. Calculate your average margin per prescription, including DIR fees. You might find that Humana plans reimburse at 3% margin while a Cigna Express Scripts plan reimburses at negative 2%. That's a $5 difference per 100 scripts.
This doesn't mean dropping plans, but it means being strategic about where you focus patient outreach and where you negotiate harder.
Second, aggressive generic cost optimization.
Generics are where most of your volume is, and they're where PBMs apply maximum pricing pressure. But generics also have the most flexibility because there are multiple suppliers and multiple routes to the same medication.
Use multiple wholesalers. National Average Drug Acquisition Cost (NADAC) pricing is published by CMS. You can access it for free. Compare your wholesaler's prices against NADAC. If you're paying 30% above NADAC on a generic, that's a negotiation opportunity.
Work with a pharmacy group or buying group that negotiates national contracts. Group Purchasing Organization (GPO) members get better rates because they have collective buying power.
And this is crucial: leverage pharmacy-to-pharmacy networks like RxPost for those medications where your wholesaler is out of stock or overpriced. RxPost customers get an average 21.8 % discount versus WAC on sourced medications. That's not $1 per script. That's meaningful margin recovery.
Third, build cash reserves specifically for DIR clawback hangover.
This sounds bleak, but it's realistic. Many PBMs aren't changing their fee structures fast enough. You might be dealing with DIR fees for years. Plan for it.
If you're running an average $8,000 to $15,000 monthly DIR costs (which is common for a mid-sized independent), budget for it. Put aside $1,500 to $2,000 per month as cash reserve. It's not pleasant, but it's honest accounting. When reform finally hits and DIR fees drop, that money becomes working capital you can redeploy.
Fourth, data-driven DIR appeals.
PBMs are legally required to provide you with the data behind their DIR fees. If a performance metric doesn't make sense or if the fee seems disproportionate, appeal it. You need documentation: "Our patient fill rate for generic ACE inhibitors was 87%, you're claiming it should be 92%. Show me the data that backs that."
Many PBMs will refund fees if you challenge them with actual documentation. It's not glamorous, but every $1,000 appeal refunded is $1,000 that stays in your business.
Fifth, network with other independent pharmacies on purchasing.
The vertical integration that's crushing us individually is a weakness when we're together. If five independent pharmacies in a region combined their purchasing power, they'd have real leverage with wholesalers and generic manufacturers. Member driven pharmacy associations facilitate this. So do informal pharmacy networks.
Get to know the three or four independent pharmacies closest to you. Share pricing information. Negotiate collective contracts. Buy generic inventory together to hit volume minimums that get you better rates. This is not collusion (that would be illegal). This is collective action for better purchasing terms.
Revenue Diversification: The Real Defense
Here's the hardest truth about PBM pressure: The solution isn't just fighting the PBM in court or lobbying Congress (though we need that too). The solution is making sure script volume and PBM reimbursement aren't 80% of your revenue.
Independent pharmacies winning in 2026 are building a diversified revenue model:
Medication Therapy Management (MTM). The American Pharmacists Association (APhA) and NCPA have resources to get certified. Medicare is expanding MTM payment. You can charge $150 to $300 per patient per year for medication reviews, adherence counseling, safety assessments. A pharmacy with 50 MTM patients generates $7,500 to $15,000 in MTM revenue that's not dependent on PBM reimbursement.
Immunizations. Every independent pharmacy should be offering flu, pneumonia, RSV, and shingles vaccines. Reimbursement is better. Patients appreciate it. It's $25 to $50 per patient per shot. A pharmacy giving 1,000 vaccines a year is generating $25,000 to $50,000 in revenue outside the PBM system.
Diabetes Self-Management Education (DSME). Similar model. Medicare and many commercial plans reimburse. You need certification, but it's achievable. One DSME patient generates $200 to $400 in revenue.
GLP-1 Counseling Services. This is emerging as a huge opportunity. Patients on semaglutide (Wegovy, Ozempic) need counseling on side effects, nutrition, medication interactions. Independent pharmacies that position themselves as GLP-1 counseling centers can charge cash for consultation ($50 to $100) or negotiate reimbursement.
Front-end optimization. This is the non-pharmacy revenue: greeting cards, supplements, OTC pain relievers, vitamins, blood pressure monitors, glucose monitors. Independents can source these more flexibly than chains. Margins are better. And they're not subject to PBM payment.
When 50% of your revenue comes from services and products outside the PBM system, a 10% reimbursement decrease hits differently. You've built redundancy.
Advocacy: Making Your Voice Heard Where It Matters
I could end this article with a framework and tactics. But the most important thing independent pharmacies can do right now is advocacy.
Real reform in states like Alabama, Idaho, and Massachusetts happened because pharmacies showed up and testified. Because patients shared stories about medication access. Because we made the problem visible to elected officials.
Here's what to do this quarter:
Join or increase your NCPA involvement. The NCPA is the national organization actually moving PBM reform legislation. They have regional chapters. Get involved in your chapter. Attend meetings. Participate in letter-writing campaigns.
Contact your state legislators directly. You don't need to be a lobbyist. You're a business owner in their district. Your letter matters. Focus on specific issues: "DIR fees cost our pharmacy $100,000 a year and force us to cut pharmacy tech hours. Is there legislation we can support?" Legislators listen to small business owners.
Share patient stories. When a patient can't get their medication because a PBM delisted your pharmacy, that's a story. When you have to counsel a patient on a less effective medication because their PBM prefers a competitor's drug, that's a story. These stories are more powerful than industry data in legislative meetings.
Join coalitions. In many states, independent pharmacies are joining coalitions with patient advocacy groups, hospitals, and consumer advocates to push for PBM reform. Look up what's happening in your state. Join.
The Oklahoma Pharmacists Association and Arkansas pharmacists have been instrumental in state-level reforms. It's not easy. But it's working.
RxPost: Reducing PBM Dependence Through Diversified Sourcing
Here's the leverage point I keep coming back to because I believe in it: Diversified sourcing reduces PBM power.
When your wholesaler is your only source, and the PBM controls what you can fill, the PBM owns you. When you have multiple sourcing channels, you have options.
RxPost is built on this principle. You connect with 600+ independent pharmacies. When you need medication that your wholesaler is out of stock on or overpricing, you source from peers. You're no longer entirely dependent on one wholesaler's inventory or pricing.
DSCSA compliance is built into the platform. The chain of custody is clean and documented. You're not taking shortcuts.
The economic impact: RxPost customers get an average 21.8% discount versus WAC. That means on a medication your wholesaler is charging $1000 for, you might source it through RxPost at $800. That's margin recovery. That's cash staying in your business instead of going to a wholesaler or PBM.
Average RxPost customers save $12,294 in the first 30 days. They recover $80.8K in surplus inventory value in 60 days. This isn't theoretical. This is happening with independent pharmacies right now.
The philosophical point matters too: When you buy from other independents, you're investing in the network that's actually competing with the chains and the PBMs. You're not strengthening a pharmaceutical distributor or a PBM. You're strengthening your peers.
Make This Actionable
Reform is happening at the federal level, but slower than we need. Reform is winning at the state level, but only in states where pharmacies organized. And you can win at your pharmacy level right now by diversifying your purchasing.
This quarter, take one step: Pull your claims data. Segment by PBM. Find the one that's costing you the most money relative to volume. Make a list of the specific DIR fees or reimbursement issues. Then schedule a meeting with your PBM account manager. Come with data. Ask specific questions. You might be surprised how much room for negotiation exists.
And set up a RxPost account. See what your surplus inventory is worth. See how many prescriptions you could fill from the pharmacy network instead of your wholesaler. This isn't replacing your wholesaler. It's building a second channel.
Take Action This Week
Contact NCPA. Visit ncpa.org. Find your state chapter. Attend a meeting. You're not committing to anything, just getting informed and getting connected.
Pull your claims data. Export your last 90 days of claims by PBM. Calculate your average margin. See where the pressure is coming from.
Create a RxPost account. It's free. List any surplus inventory. See what matches you get in the next 24 hours.
Schedule a PBM conversation. Call your account manager. Don't complain. Come with data. Ask: "Our DIR fees are $X. Can we discuss how those are calculated?"
Next Steps and Resources
The entrepreneurial pharm tech mindset doesn't accept the status quo as inevitable. It asks, "What can I change? What can I control? What leverage do I have?"
PBM reform is one of those moments where the industry is actually shifting. Take advantage of it.
Subscribe to The Entrepreneurial Pharm Tech newsletter for monthly updates on PBM reform, state legislative victories, and purchasing strategies that work. We share what's actually changing and how to position your pharmacy to benefit from it.
Follow RxPost on social (Facebook, Instagram, LinkedIn) for wins from independent pharmacies fighting back against supply chain pressure.
Join your state pharmacy association and NCPA. This is where reform happens.
Connect with us on WhatsApp for questions about purchasing strategy or surplus inventory. We're here to help.
The chains and PBMs want us to believe that this is just how it works. Here's the truth we need to say out loud together: It's not. It's changing. And you have more power than you think.
Stay Ahead with RxPost Updates
Join our newsletter to receive the latest industry insights, compliance tips, and pharmacy growth strategies straight to your inbox.
Stay Ahead with RxPost Updates
Join our newsletter to receive the latest industry insights, compliance tips, and pharmacy growth strategies straight to your inbox.
Stay Ahead with RxPost Updates
Join our newsletter to receive the latest industry insights, compliance tips, and pharmacy growth strategies straight to your inbox.
Stay Ahead with RxPost Updates
Join our newsletter to receive the latest industry insights, compliance tips, and pharmacy growth strategies straight to your inbox.
Stay Ahead with RxPost Updates
Join our newsletter to receive the latest industry insights, compliance tips, and pharmacy growth strategies straight to your inbox.
RxPost
Obsessed with delivering innovative solutions that maximize efficiencies for a healthier business.
DSCSA
Compliant
Copyright © 2026 RxPost All Right Reserved.
RxPost
Obsessed with delivering innovative solutions that maximize efficiencies for a healthier business.
DSCSA
Compliant
Copyright © 2026 RxPost All Right Reserved.
RxPost
Obsessed with delivering innovative solutions that maximize efficiencies for a healthier business.
DSCSA
Compliant
Copyright © 2026 RxPost All Right Reserved.
RxPost
Obsessed with delivering innovative solutions that maximize efficiencies for a healthier business.
DSCSA
Compliant
Copyright © 2026 RxPost All Right Reserved.
RxPost
Obsessed with delivering innovative solutions that maximize efficiencies for a healthier business.
DSCSA
Compliant
Copyright © 2026 RxPost All Right Reserved.