INDUSTRY TRENDS
PRO TIPS
Pharmacy Deserts Are Real, and Pennsylvania Just Mapped Them: What Independents Can Learn
Pharmacy Deserts Are Real, and Pennsylvania Just Mapped Them: What Independents Can Learn
Pharmacy Deserts Are Real, and Pennsylvania Just Mapped Them: What Independents Can Learn
Pharmacy Deserts Are Real, and Pennsylvania Just Mapped Them: What Independents Can Learn


I was on a call with a pharmacy owner in Pennsylvania last month when she asked me if I'd seen the pharmacy desert map. I hadn't, so she walked me through it. It's an interactive map showing which communities in Pennsylvania no longer have accessible pharmacies. Red zones. She zoomed in on her county and said, "This is getting worse. Back when I was running multiple locations five years ago, we had three independent pharmacies within five miles. Now there's one. Mine. The other two closed."
She didn't sound frustrated. She sounded scared. Because one person can't serve a community of 50,000 alone. And when she eventually retires or closes, that red zone expands.
That moment crystallized something that has been creeping up on independents for years: the pharmacy desert is real, it's growing, and it's no longer theoretical. It's happening in Pennsylvania. It's happening in Texas. It's happening in parts of California. It's happening everywhere.
Here's the truth I want us to say out loud together: pharmacy deserts aren't a Pennsylvania problem. They're a nationwide crisis playing out in slow motion. And we need to stop pretending they're inevitable. The advocacy happening right now in Pennsylvania and Alabama shows us that data plus coalition plus policy change equals real results.
Understanding Pharmacy Deserts: The Data, The Disparity, The Human Cost
Let me give you the numbers first because they matter.
Since 2020, Pennsylvania has lost more than 1,000 pharmacies. That's not a typo. Over five years, more than 1,000 independent and small chain pharmacies have closed in one state. In 2025 alone, 47 pharmacies shut down in Pennsylvania. That's up from 32 closures in 2024. The trend is accelerating.
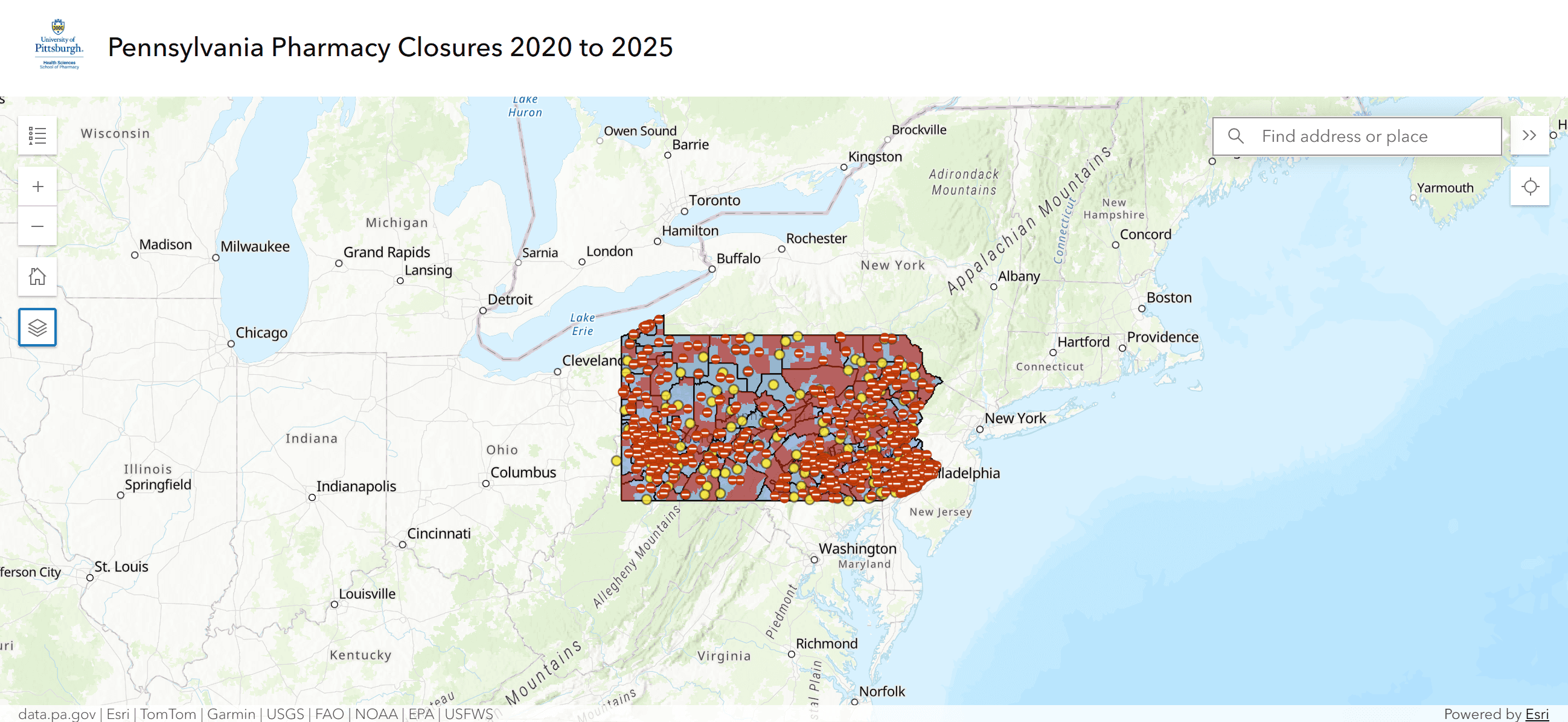
What does that look like on the ground? Communities that used to have two or three nearby pharmacies now have none. Rural areas that used to have one small independent pharmacy are now pharmacy deserts, meaning it's impossible for patients to access pharmacy services without traveling 30, 40, 50 miles.
The coalition called Pennsylvanians for Pharmacy Access created an interactive map to visualize this. You can zoom in on any zip code and see the red zones. Red means no accessible pharmacy. The map is powerful because it makes abstract numbers concrete. You can see exactly where the deserts are.
But here's what the map doesn't show clearly, and it's the most important part: the human cost.
When a community becomes a pharmacy desert, elderly patients can't get medications. Patients with chronic conditions miss doses because they can't access pharmacy services. Patients who rely on pharmacy counseling don't get it. Rural patients drive 45 minutes to fill a prescription when they used to walk ten minutes. That's not inconvenience. That's access to care being pulled away.
And here's the part that nobody talks about enough: the patients who suffer most are the poorest, the sickest, and the most rural. The patients for whom every barrier to medication access is a genuine health threat.
The pharmacy desert isn't an economic problem. It's a public health crisis.

Why PBMs Are The Core Problem
Now let's talk about why this is happening.
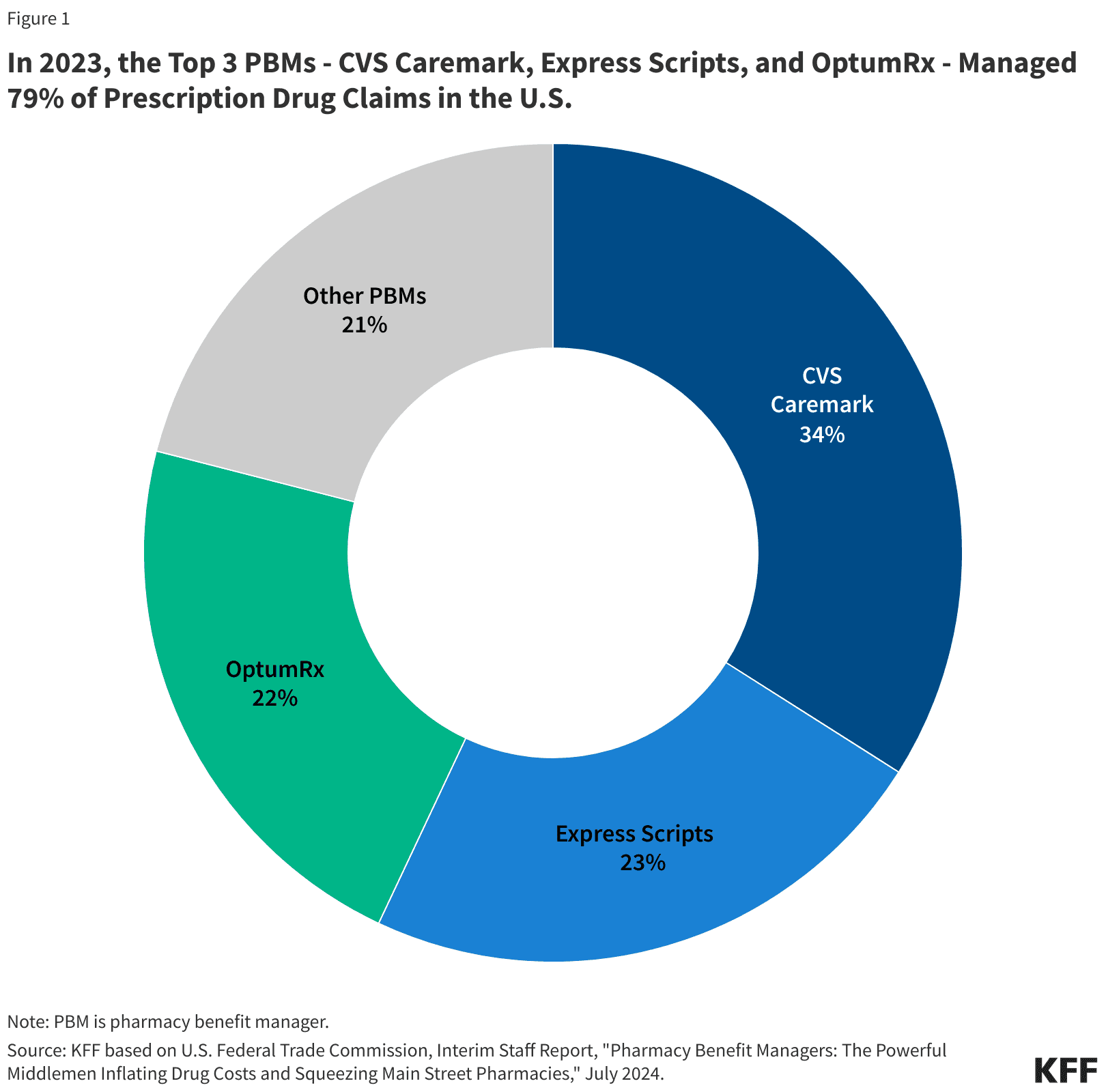
The simple answer: PBMs. The three big ones specifically. CVS Caremark, Express Scripts, and OptumRx. These three three PBMs manage nearly 80% of all prescription claims in the United States. They set the reimbursement rates that independent pharmacies receive.
Here's how the dysfunction works.
A PBM negotiates prices with drug manufacturers and with insurance companies. They're supposed to be in the middle, making the system efficient. Instead, they're extracting value at every step.
Spread pricing is one mechanism. That's when a PBM pays a pharmacy less for a drug than they charge the insurance company. The spread is pure PBM profit. A patient's insurance says, "We'll cover this drug." The PBM buys it for $50 and charges the insurance company $75. They pay the pharmacy $40. That $35 spread is PBM profit. The pharmacy absorbs a loss.
DIR fees are another mechanism. Direct and indirect remittances. A PBM charges a pharmacy fees for things like not meeting quality metrics, or having too many refills, or not dispensing according to their preferred supplier list. These fees can total thousands of dollars per pharmacy per month. An independent pharmacy with 2,000 Rxs per month might pay $5,000 to $10,000 in DIR fees.
Below-cost reimbursement is the third mechanism. A PBM reimburses a pharmacy for a medication at less than what the pharmacy paid for it. The pharmacy loses money on every fill. Most states have a minimum dispensing fee to protect against this, but the minimums are outdated and don't reflect actual costs.
The result: pharmacies can't afford to stay open. They close. And when enough pharmacies close, communities become deserts.
PBM executives will tell you that reimbursement rates are based on market forces and efficiency. That's technically true. But market forces that destroy patient access aren't efficient. They're destructive.
This is where the advocacy comes in.
The Advocacy Playbook: How Pennsylvania And Alabama Are Showing The Way
Pennsylvania has been organizing. Pennsylvanians for Pharmacy Access, as I mentioned, created the pharmacy desert map. But they also created a policy agenda. They're demanding:
Raise Medicaid dispensing fees to reflect actual pharmacy costs. Maryland and other states have done this. It's possible.
Require fair reimbursement for all pharmacies, not just those in PBM networks. If you're filling prescriptions for insured patients, you shouldn't be paid below cost.
Ban spread pricing outright. Other states are doing this. It's possible.
Transition to a single PBM for Medicaid managed care instead of letting multiple PBMs compete by squeezing pharmacies. This reduces the complexity and the pressure.
These aren't abstract demands. They're specific, achievable policy changes that would directly improve pharmacy financial sustainability.
But Pennsylvania is showing the approach, not the enforcement yet. Alabama is showing enforcement.
Alabama passed the Community Pharmacy Relief Act (Act 2025-136) and it went into effect on October 1, 2025. The law requires pharmacies to be reimbursed at least at the Medicaid reimbursement rate and bans certain fees. It also creates enforcement authority.
In December 2025, Alabama's attorney general took the first enforcement action against Express Scripts for charging illegal fees and reimbursing below the Medicaid rate. That's real accountability. That's what happens when a state says, "Enough."
Here's the critical part of the Alabama story: this is possible. A state can take action. A state can enforce consequences. Other states can watch and learn.
The advocacy playbook has three steps. First, document the problem. Second, build a coalition. Third, demand policy change and enforce it.
Pennsylvania has done steps one and two. Other states need to follow.

What Your Pharmacy Can Do Right Now
This is where I want to be very practical. You might be thinking, "This is interesting, but what can I actually do about it?"
Here's what you can do.
First: Document your own financial harm from PBM practices.
Start tracking DIR fees. Track spread pricing situations. Document months where your Medicaid reimbursement was below cost. Create a spreadsheet showing specific examples with dates, drug names, reimbursement rates, and your cost.
This matters because when your state starts building an advocacy case, they need examples from real pharmacies. Anecdotes at scale become evidence. Your documentation might be the thing that tips a legislator from "this seems like a pharmacy problem" to "this is a public health crisis."
Second: Connect with your state pharmacy association.
NCPA has state chapters. Almost every state has a state pharmacists association. These organizations are the ones building coalitions. They need to know what's happening in your pharmacy. They need to hear from pharmacists and pharmacy owners about the specific impact of PBM practices.
If you're in Pennsylvania or another state with active advocacy, join the coalition. Attend meetings. Share your story. Your voice matters because you're not abstract. You're real.
Third: Engage in public advocacy for specific policies.
This means writing letters to your state legislators about pharmacy desert mapping, about Medicaid reimbursement rates, about PBM reform. It means showing up to town halls. It means voting for candidates who support pharmacy access.
State legislatures actually listen to constituents. They listen more to constituents who show up repeatedly than to those who show up once. If you care about this, make it known to your representatives.
Fourth: Build coalition with other independents in your area.
You and the pharmacy owner two towns over are not competitors for the purposes of advocacy. You're allies. You're fighting the same PBM. You're facing the same pressure. Connect. Share your experiences. Present a united front to your state association and to policymakers.
Years of working at Roxbury Pharmacy and watching closures taught me that the pharmacy owner in Pennsylvania who I mentioned earlier, she's reached out to other independent owners in her county. They're meeting monthly. They're documenting their experiences together. They're going to present to their state representative together. That's coalition. That's powerful.
Fifth: Understand that this is also a business issue.
When a community loses pharmacies, the remaining ones become overwhelmed. Better processes, better technology, and better sourcing strategies can help you survive. RxPost can help with sourcing when you're short on inventory. Better workflows and clinical services can help you retain patients. You can't solve the PBM problem alone, but you can make your pharmacy more resilient.
The Connection Between Advocacy And Survival
I want to be clear about something: advocating for policy change isn't charity. It's survival strategy.
If pharmacy deserts expand, your pharmacy is at risk. If enough pharmacies close, you become the closest one, and the workload becomes unsustainable. If reimbursement rates don't improve, profitability for all independents suffers. Your business depends on a functional pharmacy ecosystem.
This is where entrepreneurial thinking applies to advocacy. You're not advocating for everyone else. You're advocating for the conditions you need to survive and thrive. That's business.
The Alabama pharmacy owner who worked with the attorney general on the Express Scripts enforcement action wasn't doing charity. She was protecting her business. And her action created precedent for other states.
Practical Steps To Take This Week, This Month, And This Quarter
This week: Look up your state pharmacy association and see if they have a pharmacy desert mapping project or an advocacy campaign underway. If Pennsylvania's approach has spread to your state, learn what they're doing. If it hasn't, connect with NCPA and ask about it.
This month: Spend two hours documenting one example of PBM reimbursement below cost or of DIR fees impacting your pharmacy. Get specific numbers. Get the dates. Get the drugs. Create a one-page summary. Save it. You might need it.
By end of quarter: Attend your state pharmacy association's next meeting or town hall if one is scheduled. Go prepared to share your experience. Listen to what other pharmacies are facing. Find out what advocacy is underway. Get involved.
Also, reach out to one other independent pharmacy owner in your area. Have coffee. Talk about what you're both experiencing. See if there's possibility for coalition.
The Closing Truth
The pharmacy desert is real. It's growing. And it's not inevitable. Pennsylvania is showing that data plus coalition plus policy change creates results. Alabama is showing that enforcement works. Other states can follow.
Your independent pharmacy is not just a business. It's infrastructure. It's a place where patients access healthcare. When you advocate for fair reimbursement and for pharmacy access, you're advocating for your patients and for your community.
This is where innovation meets patient care and business survival. Better advocacy equals better policy equals better conditions for independents to survive and thrive. All connected.
We are not "just filling prescriptions." We're essential healthcare providers. The pharmacy desert shouldn't exist. It exists because of policy failures, not because pharmacy isn't needed. That failure can be fixed. You can help fix it.
Start this week. Document. Connect. Advocate. That's where the power is.
Ready to Make Your Pharmacy More Resilient?
While you're advocating for systemic change, strengthen your pharmacy's financial foundation. RxPost helps independent pharmacies build resilience through strategic sourcing, giving you margin flexibility to invest in the services and infrastructure that keep you competitive.
Learn how RxPost helps independent pharmacies build resilience
I was on a call with a pharmacy owner in Pennsylvania last month when she asked me if I'd seen the pharmacy desert map. I hadn't, so she walked me through it. It's an interactive map showing which communities in Pennsylvania no longer have accessible pharmacies. Red zones. She zoomed in on her county and said, "This is getting worse. Back when I was running multiple locations five years ago, we had three independent pharmacies within five miles. Now there's one. Mine. The other two closed."
She didn't sound frustrated. She sounded scared. Because one person can't serve a community of 50,000 alone. And when she eventually retires or closes, that red zone expands.
That moment crystallized something that has been creeping up on independents for years: the pharmacy desert is real, it's growing, and it's no longer theoretical. It's happening in Pennsylvania. It's happening in Texas. It's happening in parts of California. It's happening everywhere.
Here's the truth I want us to say out loud together: pharmacy deserts aren't a Pennsylvania problem. They're a nationwide crisis playing out in slow motion. And we need to stop pretending they're inevitable. The advocacy happening right now in Pennsylvania and Alabama shows us that data plus coalition plus policy change equals real results.
Understanding Pharmacy Deserts: The Data, The Disparity, The Human Cost
Let me give you the numbers first because they matter.
Since 2020, Pennsylvania has lost more than 1,000 pharmacies. That's not a typo. Over five years, more than 1,000 independent and small chain pharmacies have closed in one state. In 2025 alone, 47 pharmacies shut down in Pennsylvania. That's up from 32 closures in 2024. The trend is accelerating.
What does that look like on the ground? Communities that used to have two or three nearby pharmacies now have none. Rural areas that used to have one small independent pharmacy are now pharmacy deserts, meaning it's impossible for patients to access pharmacy services without traveling 30, 40, 50 miles.
The coalition called Pennsylvanians for Pharmacy Access created an interactive map to visualize this. You can zoom in on any zip code and see the red zones. Red means no accessible pharmacy. The map is powerful because it makes abstract numbers concrete. You can see exactly where the deserts are.
But here's what the map doesn't show clearly, and it's the most important part: the human cost.
When a community becomes a pharmacy desert, elderly patients can't get medications. Patients with chronic conditions miss doses because they can't access pharmacy services. Patients who rely on pharmacy counseling don't get it. Rural patients drive 45 minutes to fill a prescription when they used to walk ten minutes. That's not inconvenience. That's access to care being pulled away.
And here's the part that nobody talks about enough: the patients who suffer most are the poorest, the sickest, and the most rural. The patients for whom every barrier to medication access is a genuine health threat.
The pharmacy desert isn't an economic problem. It's a public health crisis.
Why PBMs Are The Core Problem
Now let's talk about why this is happening.
The simple answer: PBMs. The three big ones specifically. CVS Caremark, Express Scripts, and OptumRx. These three three PBMs manage nearly 80% of all prescription claims in the United States. They set the reimbursement rates that independent pharmacies receive.
Here's how the dysfunction works.
A PBM negotiates prices with drug manufacturers and with insurance companies. They're supposed to be in the middle, making the system efficient. Instead, they're extracting value at every step.
Spread pricing is one mechanism. That's when a PBM pays a pharmacy less for a drug than they charge the insurance company. The spread is pure PBM profit. A patient's insurance says, "We'll cover this drug." The PBM buys it for $50 and charges the insurance company $75. They pay the pharmacy $40. That $35 spread is PBM profit. The pharmacy absorbs a loss.
DIR fees are another mechanism. Direct and indirect remittances. A PBM charges a pharmacy fees for things like not meeting quality metrics, or having too many refills, or not dispensing according to their preferred supplier list. These fees can total thousands of dollars per pharmacy per month. An independent pharmacy with 2,000 Rxs per month might pay $5,000 to $10,000 in DIR fees.
Below-cost reimbursement is the third mechanism. A PBM reimburses a pharmacy for a medication at less than what the pharmacy paid for it. The pharmacy loses money on every fill. Most states have a minimum dispensing fee to protect against this, but the minimums are outdated and don't reflect actual costs.
The result: pharmacies can't afford to stay open. They close. And when enough pharmacies close, communities become deserts.
PBM executives will tell you that reimbursement rates are based on market forces and efficiency. That's technically true. But market forces that destroy patient access aren't efficient. They're destructive.
This is where the advocacy comes in.
The Advocacy Playbook: How Pennsylvania And Alabama Are Showing The Way
Pennsylvania has been organizing. Pennsylvanians for Pharmacy Access, as I mentioned, created the pharmacy desert map. But they also created a policy agenda. They're demanding:
Raise Medicaid dispensing fees to reflect actual pharmacy costs. Maryland and other states have done this. It's possible.
Require fair reimbursement for all pharmacies, not just those in PBM networks. If you're filling prescriptions for insured patients, you shouldn't be paid below cost.
Ban spread pricing outright. Other states are doing this. It's possible.
Transition to a single PBM for Medicaid managed care instead of letting multiple PBMs compete by squeezing pharmacies. This reduces the complexity and the pressure.
These aren't abstract demands. They're specific, achievable policy changes that would directly improve pharmacy financial sustainability.
But Pennsylvania is showing the approach, not the enforcement yet. Alabama is showing enforcement.
Alabama passed the Community Pharmacy Relief Act (Act 2025-136) and it went into effect on October 1, 2025. The law requires pharmacies to be reimbursed at least at the Medicaid reimbursement rate and bans certain fees. It also creates enforcement authority.
In December 2025, Alabama's attorney general took the first enforcement action against Express Scripts for charging illegal fees and reimbursing below the Medicaid rate. That's real accountability. That's what happens when a state says, "Enough."
Here's the critical part of the Alabama story: this is possible. A state can take action. A state can enforce consequences. Other states can watch and learn.
The advocacy playbook has three steps. First, document the problem. Second, build a coalition. Third, demand policy change and enforce it.
Pennsylvania has done steps one and two. Other states need to follow.
What Your Pharmacy Can Do Right Now
This is where I want to be very practical. You might be thinking, "This is interesting, but what can I actually do about it?"
Here's what you can do.
First: Document your own financial harm from PBM practices.
Start tracking DIR fees. Track spread pricing situations. Document months where your Medicaid reimbursement was below cost. Create a spreadsheet showing specific examples with dates, drug names, reimbursement rates, and your cost.
This matters because when your state starts building an advocacy case, they need examples from real pharmacies. Anecdotes at scale become evidence. Your documentation might be the thing that tips a legislator from "this seems like a pharmacy problem" to "this is a public health crisis."
Second: Connect with your state pharmacy association.
NCPA has state chapters. Almost every state has a state pharmacists association. These organizations are the ones building coalitions. They need to know what's happening in your pharmacy. They need to hear from pharmacists and pharmacy owners about the specific impact of PBM practices.
If you're in Pennsylvania or another state with active advocacy, join the coalition. Attend meetings. Share your story. Your voice matters because you're not abstract. You're real.
Third: Engage in public advocacy for specific policies.
This means writing letters to your state legislators about pharmacy desert mapping, about Medicaid reimbursement rates, about PBM reform. It means showing up to town halls. It means voting for candidates who support pharmacy access.
State legislatures actually listen to constituents. They listen more to constituents who show up repeatedly than to those who show up once. If you care about this, make it known to your representatives.
Fourth: Build coalition with other independents in your area.
You and the pharmacy owner two towns over are not competitors for the purposes of advocacy. You're allies. You're fighting the same PBM. You're facing the same pressure. Connect. Share your experiences. Present a united front to your state association and to policymakers.
Years of working at Roxbury Pharmacy and watching closures taught me that the pharmacy owner in Pennsylvania who I mentioned earlier, she's reached out to other independent owners in her county. They're meeting monthly. They're documenting their experiences together. They're going to present to their state representative together. That's coalition. That's powerful.
Fifth: Understand that this is also a business issue.
When a community loses pharmacies, the remaining ones become overwhelmed. Better processes, better technology, and better sourcing strategies can help you survive. RxPost can help with sourcing when you're short on inventory. Better workflows and clinical services can help you retain patients. You can't solve the PBM problem alone, but you can make your pharmacy more resilient.
The Connection Between Advocacy And Survival
I want to be clear about something: advocating for policy change isn't charity. It's survival strategy.
If pharmacy deserts expand, your pharmacy is at risk. If enough pharmacies close, you become the closest one, and the workload becomes unsustainable. If reimbursement rates don't improve, profitability for all independents suffers. Your business depends on a functional pharmacy ecosystem.
This is where entrepreneurial thinking applies to advocacy. You're not advocating for everyone else. You're advocating for the conditions you need to survive and thrive. That's business.
The Alabama pharmacy owner who worked with the attorney general on the Express Scripts enforcement action wasn't doing charity. She was protecting her business. And her action created precedent for other states.
Practical Steps To Take This Week, This Month, And This Quarter
This week: Look up your state pharmacy association and see if they have a pharmacy desert mapping project or an advocacy campaign underway. If Pennsylvania's approach has spread to your state, learn what they're doing. If it hasn't, connect with NCPA and ask about it.
This month: Spend two hours documenting one example of PBM reimbursement below cost or of DIR fees impacting your pharmacy. Get specific numbers. Get the dates. Get the drugs. Create a one-page summary. Save it. You might need it.
By end of quarter: Attend your state pharmacy association's next meeting or town hall if one is scheduled. Go prepared to share your experience. Listen to what other pharmacies are facing. Find out what advocacy is underway. Get involved.
Also, reach out to one other independent pharmacy owner in your area. Have coffee. Talk about what you're both experiencing. See if there's possibility for coalition.
The Closing Truth
The pharmacy desert is real. It's growing. And it's not inevitable. Pennsylvania is showing that data plus coalition plus policy change creates results. Alabama is showing that enforcement works. Other states can follow.
Your independent pharmacy is not just a business. It's infrastructure. It's a place where patients access healthcare. When you advocate for fair reimbursement and for pharmacy access, you're advocating for your patients and for your community.
This is where innovation meets patient care and business survival. Better advocacy equals better policy equals better conditions for independents to survive and thrive. All connected.
We are not "just filling prescriptions." We're essential healthcare providers. The pharmacy desert shouldn't exist. It exists because of policy failures, not because pharmacy isn't needed. That failure can be fixed. You can help fix it.
Start this week. Document. Connect. Advocate. That's where the power is.
Ready to Make Your Pharmacy More Resilient?
While you're advocating for systemic change, strengthen your pharmacy's financial foundation. RxPost helps independent pharmacies build resilience through strategic sourcing, giving you margin flexibility to invest in the services and infrastructure that keep you competitive.
Learn how RxPost helps independent pharmacies build resilience
Stay Ahead with RxPost Updates
Join our newsletter to receive the latest industry insights, compliance tips, and pharmacy growth strategies straight to your inbox.
Stay Ahead with RxPost Updates
Join our newsletter to receive the latest industry insights, compliance tips, and pharmacy growth strategies straight to your inbox.
Stay Ahead with RxPost Updates
Join our newsletter to receive the latest industry insights, compliance tips, and pharmacy growth strategies straight to your inbox.
Stay Ahead with RxPost Updates
Join our newsletter to receive the latest industry insights, compliance tips, and pharmacy growth strategies straight to your inbox.
Stay Ahead with RxPost Updates
Join our newsletter to receive the latest industry insights, compliance tips, and pharmacy growth strategies straight to your inbox.
RxPost
Obsessed with delivering innovative solutions that maximize efficiencies for a healthier business.
DSCSA
Compliant
Copyright © 2026 RxPost All Right Reserved.
RxPost
Obsessed with delivering innovative solutions that maximize efficiencies for a healthier business.
DSCSA
Compliant
Copyright © 2026 RxPost All Right Reserved.
RxPost
Obsessed with delivering innovative solutions that maximize efficiencies for a healthier business.
DSCSA
Compliant
Copyright © 2026 RxPost All Right Reserved.
RxPost
Obsessed with delivering innovative solutions that maximize efficiencies for a healthier business.
DSCSA
Compliant
Copyright © 2026 RxPost All Right Reserved.
RxPost
Obsessed with delivering innovative solutions that maximize efficiencies for a healthier business.
DSCSA
Compliant
Copyright © 2026 RxPost All Right Reserved.